Antiplatelets are a group of medicines that stop blood cells (called platelets or thrombocytes) from sticking together and forming a blood clot.
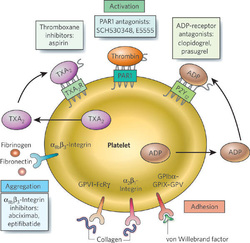
The body sends platelets to the site of the injury, where these cells clump together to form a blood clot and stop the bleeding. This is good for a cut or a wound, but not for an injured (inflamed, with plague build-ups or devices placed inside - like stents) blood vessel. Antiplatelet medicines are taken to stop blood clots from forming by attacking different factors contributing to this process - activation of platelets, adhesion or aggregation.
The body sends platelets to the site of the injury, where these cells clump together to form a blood clot and stop the bleeding. This is good for a cut or a wound, but not for an injured (inflamed, with plague build-ups or devices placed inside - like stents) blood vessel. Antiplatelet medicines are taken to stop blood clots from forming by attacking different factors contributing to this process - activation of platelets, adhesion or aggregation.
- Aspirin is the most common type of antiplatelet medicine. It is a weak inhibitor of platelet aggregation compared to other antiplatelet drugs and typically is used in combination with other antiplatelet drugs. It has been the drug of choice for many years and is still a common drug. Low-dose aspirin (sometimes called "baby aspirin") may prevent heart attacks and strokes in people who take it every day. It is conveniently dosed for once a day and recommended to be taken with food to decrease gastrointestinal side effects.
- Adenosine diphosphate (ADP) receptor inhibitors are usually given to patients who have had a recent heart attack or stroke, because these patients have a greater risk of having another heart attack or stroke. Doctors may also give this medicine to patients with mitral valve disease or those who have had heart valve replacement. Some patients with peripheral vascular disease (PVD) may also be good candidates for ADP receptor inhibitors, because poor blood circulation in the legs can lead to blood clots. Examples are: clopidogrel, prasugrel, ticlopidine, ticagrelor, cangrelor, and elinogrel. There are concerns about decreased efficacy if clopidogrel is administered in poor metabolizers, specifically with the CYP2C19*2 or CYP2C19*3 alleles. Prasugrel is the newest thienopyridine drug and does not have similar concerns of decreased efficacy in patients who are poor metabolizers or are on concurrent PPIs.
- Adenosine reuptake inhibitors are usually given to patients in combination with an anticoagulant. Patients may also take this type of antiplatelet therapy in combination with aspirin if they have a heart condition that increases their risk of blood clots.
- Glycoprotein IIB/IIIA inhibitors are given by an intravenous (IV) needle directly into the bloodstream, so patients must be in the hospital to receive them. Patients usually receive this type of antiplatelet medicine to prevent blood clots that sometimes form during angioplasty and stent procedures. They are also used in patients with angina who are going to have an angioplasty or stent procedure. Currently, three different agents for intravenous use are in clinical use. The first, abciximab, is a chimeric antibody that irreversibly binds and inactivates the glycoprotein IIb/IIIa receptor (whose activation is the final common pathway in platelet activation). The other two, tirofiban and eptifibatide, are non‐antibody agents that competitively bind the glycoprotein IIb/IIIa receptor.
- Phosphodiesterase inhibitors is most often used in patients with PVD to reduce leg pain that comes with walking (called intermittent claudication). Patients with PVD have a greater risk of developing blood clots in their legs, so some PVD patients need to take antiplatelet medicines. Patients with heart failure should not take this type of antiplatelet medicine, because studies have shown it can lead to death.