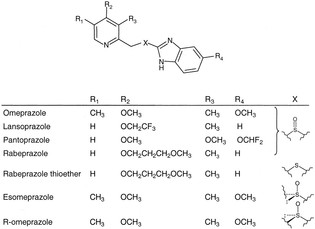
Drugs reducing the amount of acid made by the stomach. Proton Pump Inhibitors (PPIs) work by binding to protein pumps (hydrogen/potassium ATPase enzymes on gastric parietal cells) and blocking the secretion of hydrogen ions into the stomach, which combine with chloride ions in the stomach lumen to form gastric acid. PPIs are used to treat heartburn, gastroesophageal reflux disease (GERD), and gastric ulcers. Two most common uses of PPIs are treatment of dyspepsia and prevention of gastrointestinal bleeding among patients prescribed antiplatelet therapy.